Here, also add:
Mary Smith (Chart ID Mary has access to)
Because Mary Smith could also be a patient in the practice, along with Bill Jones.
Your idea would still work though, right?
There would just be two entries (or more, if needed) in the linking table, right? One for her own chart, one for Bill Jones chart.
No it’d be more along the lines of a provider login. From this log in, patient data would be only from a set of patients the provider is authorized to see. I think care team would be great for this.
In Occupational Health almost always, the company is self insured or manage insurance, OSHA and other regulatory agency requirements concerning patients/employees. The capability to log in and check drug screens, labs, notes etc is ideal.
I know, it makes it simpler to provide the information, without having to generate a report, printing it and mailing it; or generating a report, downloading it and uploading it into the WC FTP. If everything could be done from the OpenEMR interface, it would be awesome!
I believe this is necessary though. You don’t want a patient-portal-user profile to be a medical record user. The distinction is very important.
Also, access to care-team members could be temporary. For example, often insurance companies want patient records because they want to know if the provider has achieved certain care measures. The access could be approved temporarily. This would be a different interface though. I think the wordpress portal would work in this context.
A number of other systems resolve this through ACLs as the identity provider user service is separate from the user-type or user-role. Having the separate tables provides an additional safety check that patients are not inadvertently mixed in with clinicians. The downside is what we are facing right now is both the duplication and decentralization of both authorization and authentication systems.
For example right now there is no way in the system to provide a more restricted subset of data to a representative of a patient that the patient has authorized to have access to only that subset of data. With FHIR the patient could sort-of hack this by granting a 3rd party app certain resource scopes (for example access to just their immunization and allergy information) and then share their account credentials to their authorized representative, but that is pretty hacky in my opinion.
Anyways, food for thought, the codebase is open and available and we welcome people contributing whether that be documentation or code.
Hmmm, I wonder how Postgresql does it.
Would it help if OpenEMR switched to a database that could help it handle its authorizations?
Or how about an authorizations table? Don’t all entries in OpenEMR have a unique ID?
Alright, I will stop, this is not even a documentation thing!
Yea, fun thread, you should jump on our Saturday call (probably not this saturday (July 3rd 2021) as I doubt with the holiday many people will be on) and we can talk about database design if you want.
Would appreciate any beta- readers, so to speak, to proof it for errors and omissions.
Also-- has anybody heard of OpenEMR v6+ having an alternate (maybe a numeric pin?) method of e-signing documents besides the mouse- scrawled graphic sig? I thought I read of it here somewhere but now can’t find it. I do know it has a pin for staff to e-sign clinical forms, but I’m thinking of something available to patients in the portal. If so, can you steer me towards that info?
In any case I’m starting on an overview of the Patient Portal in OpenEMR v6+ and definitely want to mention the alternate e-sig there, if it exists.
Best- Harley
There’s also a lot of good information on youtube. But only a small fraction is posted to the official OpenEMR youtube itself. A lot of videos seem to be recorded and uploaded by vendors or on a personal youtube account.
I think @juggernautsei may have recorded a video on nation notes capability.
@Rachel_Ellison
The video I did years ago is not accurate any longer. @sjpadgett has taken nations note and spread it all over the system to any text box in any form.
you can watch the nations note video I did to help build context. However, nations note no longer has to be installed. Just open the current soap note and double-click in the text area. You will see a popup that is the nation’s note feature. You can then create a context and assign stored phrases for that text area so you can build notes.
Yes, I am already using it. It is quite good and opens automatically upon clicking on any text area. I am still getting the hang of adding the categories and other parts of it.
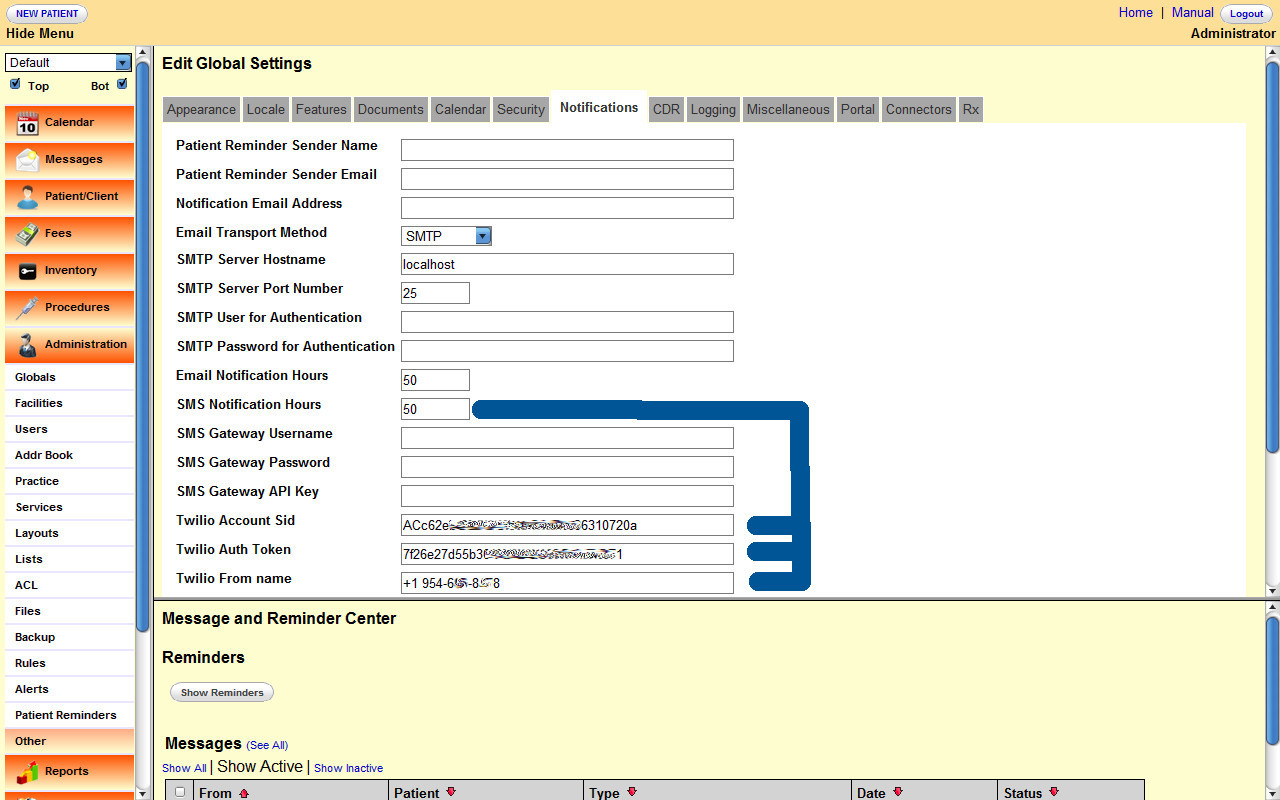
I am still not finding information on how to set up SMS. Is it possible someone could kindly post an image of how their notifications page in globals is configured? Honestly, the documentation is outdated.
I can update it, but I need to be able to set up my system, or see someone else’s example.
Also, do I need a separate twilio interface?
Twilio is giving me and account SID and auth token. How are these fields related to the fields in openemr notifications configuration page?
@gutiersa
The image you posted, I just seen it. Reposting it here. This goes with BatchComm Tools.
You can use any SMS provider. It does not have to be Twillio.